
(9 min read) Once upon a time, in a land far, far away, a communications center worker answered an emergency call from a caller who relayed that her husband had collapsed

(9 min read) Once upon a time, in a land far, far away, a communications center worker answered an emergency call from a caller who relayed that her husband had collapsed. The call taker carefully wrote down the call-back number (there was no Automated Number Identification) and address of the emergency (there was no Automated Location Identification). With only her experience as a guide, the call taker asked a series of questions and dispatched police, fire, and an ambulance (from the local funeral home — which also ran the ambulance service), and the units responded. The time of call, dispatch, arrival, transporting, and at-destination times were handwritten in the dispatch log.
Seem unimaginable? Not so much – many early emergency communications centers operated not too differently. When you think about how far we’ve come in emergency communications centers, imagine what’s in store for the future!
The Emergency Medical Services (EMS) delivery model is transforming at a rate never before experienced. Much of this rapid transformation is due to the ongoing Public Health Emergency (PHE) related to the COVID-19 pandemic. What many of us thought might take 20 years to evolve took 20 months! EMS providers are doing much more than simply responding to emergency calls and transporting patients to an emergency department (ED). EMS agencies are treating patients who access EMS through 911 with low-acuity medical issues in their homes instead of transporting patients to EDs if they do not need to go there. They are managing high-risk patients proactively to prevent a 911 call. They are partnering with payers, home health, and hospice agencies to reduce preventable ED visits. And, they’re administering vaccines and providing monoclonal antibody (mAb) infusions.
For the past 50 years, the basic economic model for EMS was relatively unchanged: you call, we haul, we get paid (maybe). Generally, EMS agencies are paid when they transport patients to the ED; however, many EMS agencies are testing new economic models with payers and other partners that reimburse them for NOT taking patients to the ED.
The crucial role communications centers play amidst dynamic changes taking place in EMS delivery and economic models cannot be understated. Activities within the comm center impact responder safety, resource deployment and allocation, and patient outcomes. It’s where the response begins, and it serves as the central point for determining which resources respond, how they respond, and even if they respond. Here’s how:
Responder Safety
One of the highest risks to emergency responders are crashes that result when emergency vehicles operate in an emergency mode, lights and siren, or “HOT” operation. Reducing HOT responses saves lives of responders and the public. Emergency Medical Dispatch (EMD) systems can effectively and presumptively determine whether a HOT response will make a difference in the patient’s outcome and justify the increased risk of crashes. For example, a HOT response may be warranted in the case of a 6-year-old who received an accidental gunshot wound to the abdomen. Conversely, a HOT response may not be warranted in the case of a 45-year-old female who slipped and twisted her ankle. Comm centers should work with EMS agency directors and medical directors to carefully review dispatch processes and do everything reasonably possible to reduce HOT EMS responses.
![Response-Determinant-Methodology-Response-Code-Matrix-showing-local-response-examples[1]](https://www.zolldata.com/hs-fs/hubfs/Response-Determinant-Methodology-Response-Code-Matrix-showing-local-response-examples%5B1%5D.png?width=495&name=Response-Determinant-Methodology-Response-Code-Matrix-showing-local-response-examples%5B1%5D.png)
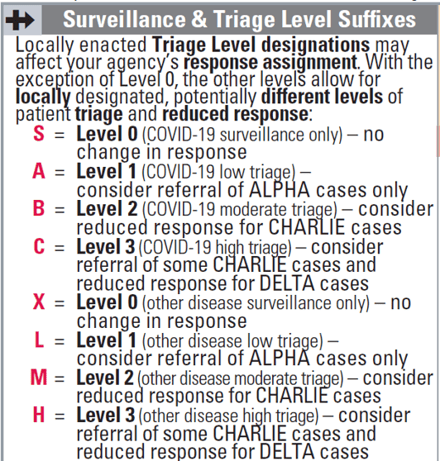
Similarly, during the PHE, many comm centers implemented enhanced screening protocols to try and identify if a patient is at high risk for COVID-19. The “36 Protocol” by Medical Priority Solutions® was designed to walk the call-taker through a series of specific questions to assess pandemic risk. When used by the comm center, responses for patients who seems to be at risk for a COVID infections can be communicated to responders, urging them to use extra infectious disease precautions prior to entering the scene. In some comm centers, protocols were implemented that used this protocol to advise very low-acuity 911 callers that their medical condition did not necessitate an EMS response. Instead, the call taker provided the caller with information about how to access resources for their medical care.
Resource Allocation
Not all EMS requests are created equal, and while some may be for life-threatening emergencies, many are for low-acuity medical complaints. Using an effective EMD program combined with a bit of data analytics can change how EMS responds to medical calls. Calls with a high probability of an acute, life-threatening medical emergency can receive one type of response, while calls for things like a twisted ankle can receive a different response. For the former, a maximal response by first responders and ambulance personnel driving HOT may make a difference in the patient’s outcome. For the ankle injury, a COLD response from an ambulance only may be most appropriate.
Let’s take that process one transformative step further. Suppose a detailed analysis of isolated ankle injury calls for patients under 60 years old reveals that 79% of the time, these patients are not transported to an ED. Perhaps there is no need to send an ambulance at all. Maybe first responders or an EMS Quick Response Vehicle (QRV) with a single paramedic could respond for an initial assessment. If it is determined that the patient needs to go to the ED, the ambulance can be dispatched. Conducting this type of detailed analysis for all response determinants could lead to a major shift in resource allocation, with first responders or a QRV only responding to a select number of EMS calls that have a low transport percentage. With the current EMS worker shortage, changes like this can reduce the ambulance resources needed to cover the EMS needs of the community.
Resource Deployment
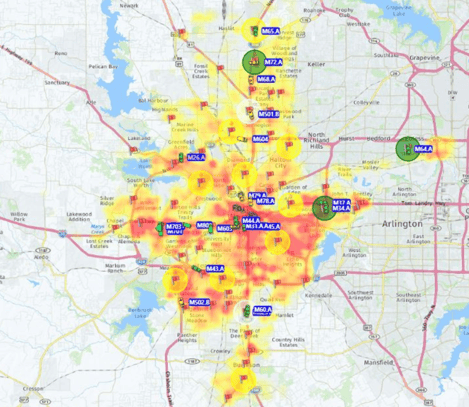
EMS response volumes predictably fluctuate during a typical day, with more calls occurring when people are awake, commuting, or recreating on the weekends than when most people are home sleeping. EMS responses also tend to follow populations movement since EMS responses are for a person as opposed to a response for a fire incident, which is generally a response to a fixed structure. For example, take a typical core city with a few adjoining, residential suburbs. During the workday, response volumes will generally be higher in the core city, since many of the people residing in the suburbs may travel into the city to work or play. During evenings and weekends, the response volume may be higher in the suburbs when people shift to residential areas.
It makes sense that EMS resources be shifted (or deployed) from areas with low anticipated response volumes to areas with higher anticipated response volumes. This concept is called Dynamic Resource Management and moves EMS resources to geographic areas at specific times of day based on historical response volumes based on time of day and day of week.
Since the response volumes change throughout a 24-hour period, it also makes sense to staff more ambulances during high volume time periods and fewer during slow call volume periods. Response data from the comm center is a vital tool to making these resource allocation and deployment strategies.
Custom Designed, Patient-Specific Response Plans
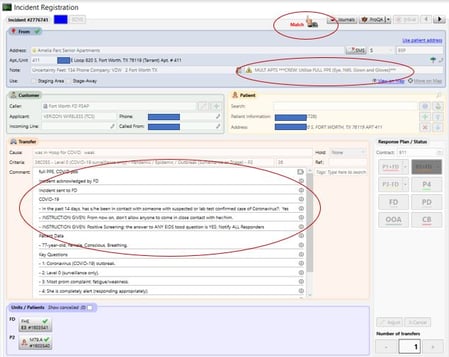
Much like address flags in computer aided dispatch (CAD) systems, a transformed EMS comm center can flag patients, not just addresses. When a 911 caller accesses the EMS comm center, the call taker can ask the patient’s name and date of birth and match it to a patient database in the CAD. A match can lead to a specialized response plan for that individual patient. For example, some EMS organization have partnered with hospice agencies to help prevent an avoidable ED visit for a hospice-related plan of care incident. The hospice agency provides the EMS comm center with a list of their patients to flag in the CAD. During the 911 call taking process, the call taker asks the patient’s name and date of birth. This information, if matched to a patient in the CAD database, results in a response plan built specifically for THAT patient. The response plan can be to notify the hospice agency about the response and to add to the response a community paramedic to assist with on-scene patient navigation.
The same concept can be applied to members of a specific payer group that has contracted with EMS to pay them for not transporting a member to the ED. For example, the EMS agency contracts with ACME Health Insurance for a fixed payment each month, based on the number of their insured members in the EMS agency’s service area. The EMS agency is no longer required to transport the insured member to an ED to get paid for their services. The payer provides a monthly list of their members in the EMS agency’s service area and this data is uploaded each month into the comm center CAD. When an ACME-insured member calls 911, the member’s name is matched in CAD. The responding ambulance crew is notified that, if clinically appropriate, the patient they are responding to can be navigated to resources other than an ED since the EMS agency has already been paid for their services. This arrangement provided enhanced value to the patient, the insurance company, and the EMS agency.
Telehealth FROM the EMS Comm Center
The Centers for Medicare and Medicaid Services (CMS) has issued a series of waivers that make telehealth services more accessible for patients, and many EMS agencies have partnered with telehealth providers to assist with Treatment in Place (TIP) services, without the need for an EMS transport to an ED. The on-scene EMS agency caring for a low-acuity patient engages a telehealth agency to provide enhanced patient assessment and navigation to avoid the ED. There is no reason, however, that service can’t be provided by the EMS comm center at the point of a 911 call. For example, a call is received for a patient complaining of low-acuity leg pain and the EMD determinant for the call meets medical director approved criteria for telehealth. The EMS comm center could send the caller a text message with a link to access a telehealth provider to their smart device. The EMS comm center stays on the line while the physician engages with the patient. At the end of the encounter, the physician orders a medication from a local pharmacy and recommends the patient visit their primary care physician in the next 24 to 48 hours. No EMS “response” occurs, saving precious resources while getting the patient the care they require. Under a waiver issued by CMS for the PHE, the telehealth physician is reimbursed by Medicare or other payers and in turn, can pay the EMS comm center for facilitating the telehealth intervention.
Do all these transformed services sound crazy and unrealistic? Well, they are happening today! Every one of the transformed service examples I’ve shared is currently being provided by EMS comm centers in communities across the country.
The key to transitioning from a traditional to a transformed EMS comm center is envisioning the future state, using data to drive decisions, and partnering with the right technology provider and medical director to enhance the value of the comm center in the EMS delivery system.
Read More About the EMS Industry Transformation:
COVID, Competition, and the Cloud Push the Industry Toward EMS 4.0
Want to Receive the ZOLL Pulse Blog in Your Inbox? Subscribe.
ZOLL Pulse Blog
Subscribe to our blog and receive quality content that makes your job as an EMS & fire, hospital, or AR professional easier.
ZOLL Pulse Blog
Subscribe to our blog and receive quality content that makes your job as an EMS, fire, hospital, or AR professional easier.

